

ACL injuries remain one of the most devastating injuries in soccer, and despite decades of research, incidence has not meaningfully dropped.
- 6–23% increase over the past two decades
- 14–20x more likely during matches than training
- Only ~54–65% return to their previous level 3–4 years later
This study aimed to synthesize all high-level video analysis research (13 studies and 709 ACL) to answer a simple but powerful question:
What are the most common mechanisms, patterns, and biomechanics of ACL injuries in soccer?
What Did the Researchers Do?
The researchers conducted a systematic review and meta-analysis in accordance with PRISMA guidelines.
- 13 studies (2015–2024)
- 709 ACL injuries
- 614 male, 95 female players
- Mostly professional players
- Video-analysis only
The researchers extracted:
- Injury mechanism (non-contact, direct, indirect)
- Playing situation (attacking vs defending)
- Ball possession
- Specific action (pressing, cutting, landing, etc.)
- Leg support (single vs double)
- Horizontal & vertical velocity
- Biomechanics at initial Contact (IC) and injury Frame (IF)
What Were the Results?
Mechanism is Mostly Non-Contact
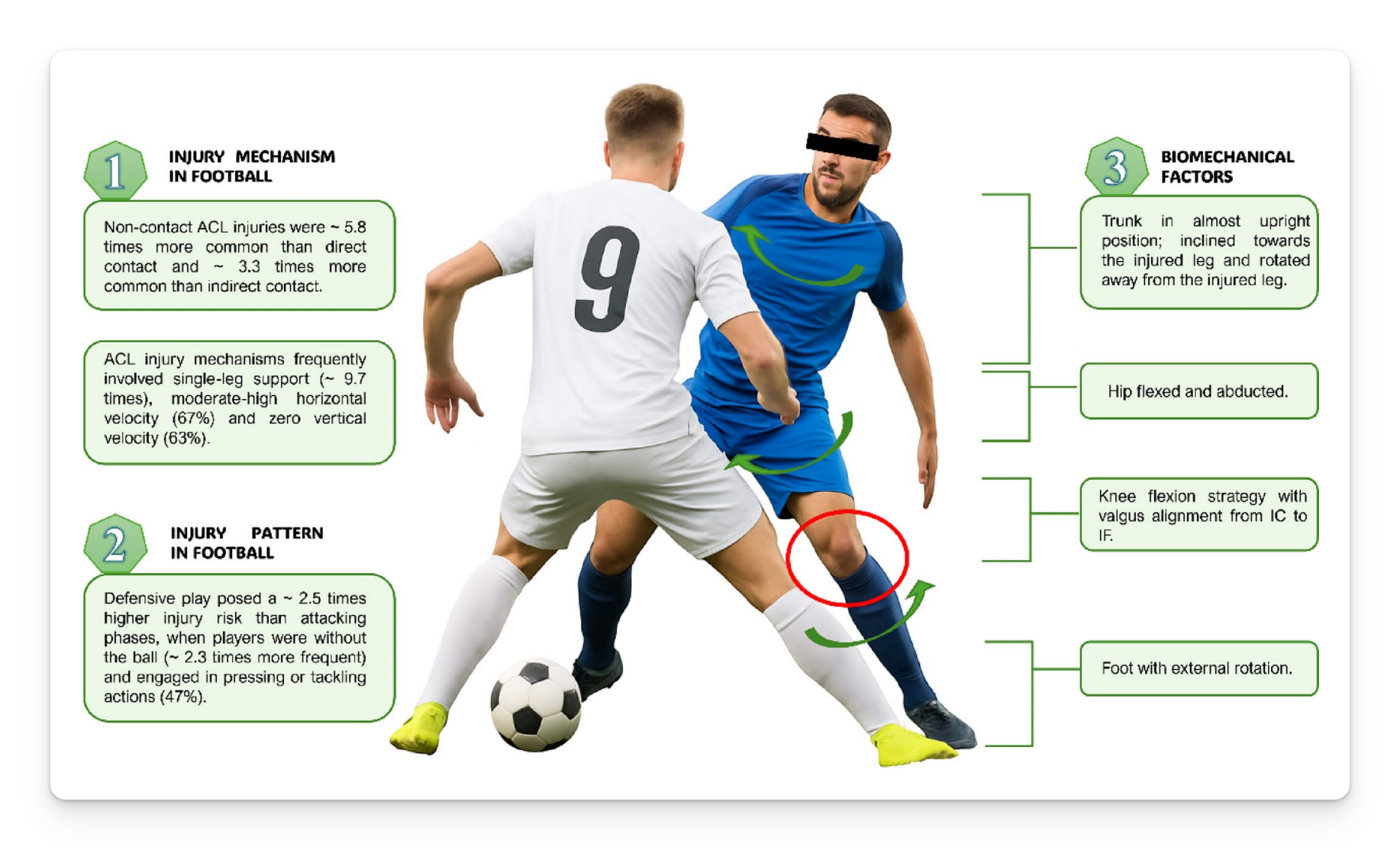
- Non-contact injuries were 5.75x more likely than direct contact and 3.32x more likely than indirect contact
- Similar trend in males and females
- In females, indirect contact was more common than direct contact
This confirms what we see: most ACLs rupture without major collision.
Defensive Actions Dominate
- Defending injuries were 2.5x more likely than attacking injuries
- Injuries without ball possession were 2.3x more likely
- 47% occurred during pressing/tackling
Most ACL injuries happen when reacting to someone else.
Single-Leg Support Is the Big Risk Context
- Single-leg support injuries were 9.66x more likely than double-leg support injuries
- 69% occurred on one leg
- Most happened at moderate-to-high horizontal velocity
- 63% occurred with zero vertical velocity
ACL injuries in soccer are primarily a braking problem, not a landing problem.
Biomechanical Pattern
At Initial Contact (IC):
- Knee flexion ≈ 26°
- Hip flexion ≈ 36°
- Trunk nearly upright
- Hip abducted (73%)
- Foot externally rotated (51%)
At Injury Frame (IF):
- Knee flexion ≈ 39°
- Knee valgus in 79% of cases
- Hip abducted (76%)
- Trunk rotated away from injured leg (61%)
This is a multi-planar collapse during deceleration.
Timing Matters
- More injuries in the first 45 minutes
- Peaks in September–November and February–April
- This suggests load spikes and seasonal transitions may matter more than late-game fatigue.
What Does This Mean?
ACL injuries in soccer typically look like this:
- Defensive action
- No ball possession
- Moderate-to-high horizontal speed
- Single-leg braking
- Trunk rotated
- Hip abducted
- Knee flexed with valgus
Importantly, ACL injuries are not just a “valgus issue." They result from an interaction among speed, reactivity, contact, and mechanics.
ACL injury is complex and should be interpreted holistically.
Limitations
- High heterogeneity across studies
- Mostly male professional players (85%)
- Possible overlapping datasets
- Variation in video quality and reporting
Coach’s Takeaway
- Train high-speed single-leg deceleration under pressure ⮕ Build braking capacity at moderate to high horizontal velocities
- Prioritize defending-specific prevention work ⮕ Use reactive, chaotic drills that include realistic upper-body contact
- Go beyond cueing “no valgus” ⮕ Improve trunk control, hip strength, and deceleration mechanics at game speed
ACL prevention is not a checklist; it should prepare players for the exact scenarios where injuries actually occur.
I hope this helps,
Ramsey
Reference: Miralles-Iborra A, Vera-Garcia FJ, Elvira JLL, et al. (2025). Mechanisms, Injury Patterns and Biomechanical Factors of Anterior Cruciate Ligament Injuries in Football (Soccer): A Systematic Review and Meta-Analysis of Video-Analysis Studies. Sports Medicine.


