

Achilles tendon rupture (ATR) has long-term consequences.
Even years after injury, we see reduced plantarflexion strength, reduced ankle power and persistent performance asymmetries.
The authors wanted to understand whether lower leg muscles are activated differently one year post-ATR and how each muscle contributes to ankle plantarflexion work during single-leg hopping.
This study is a good reminder that programming needs to target mechanical efficiency, especially during rehab.
Why is plantarflexion power still down one year after Achilles rupture, and which muscles are actually doing the work?
What Did the Researchers Do?
Participants
This was a cross-sectional study of 37 individuals at 1-year post-Achilles rupture.
- Mean age: 48 years
- 65% underwent surgery
- Compared affected vs unaffected limb
Testing
Participants performed 25 continuous single-leg hops per limb with:
- 3D motion capture
- Force plates
- Surface EMG
Muscles Recorded
- Soleus (SOL)
- Tibialis anterior (TA)
- Lateral gastrocnemius (GL)
- Medial gastrocnemius (GM)
All EMG was normalized to MVIC.
Outcomes Measured
- Sagittal ankle power
- Plantarflexion work (time-integrated power)
- Muscle activation patterns
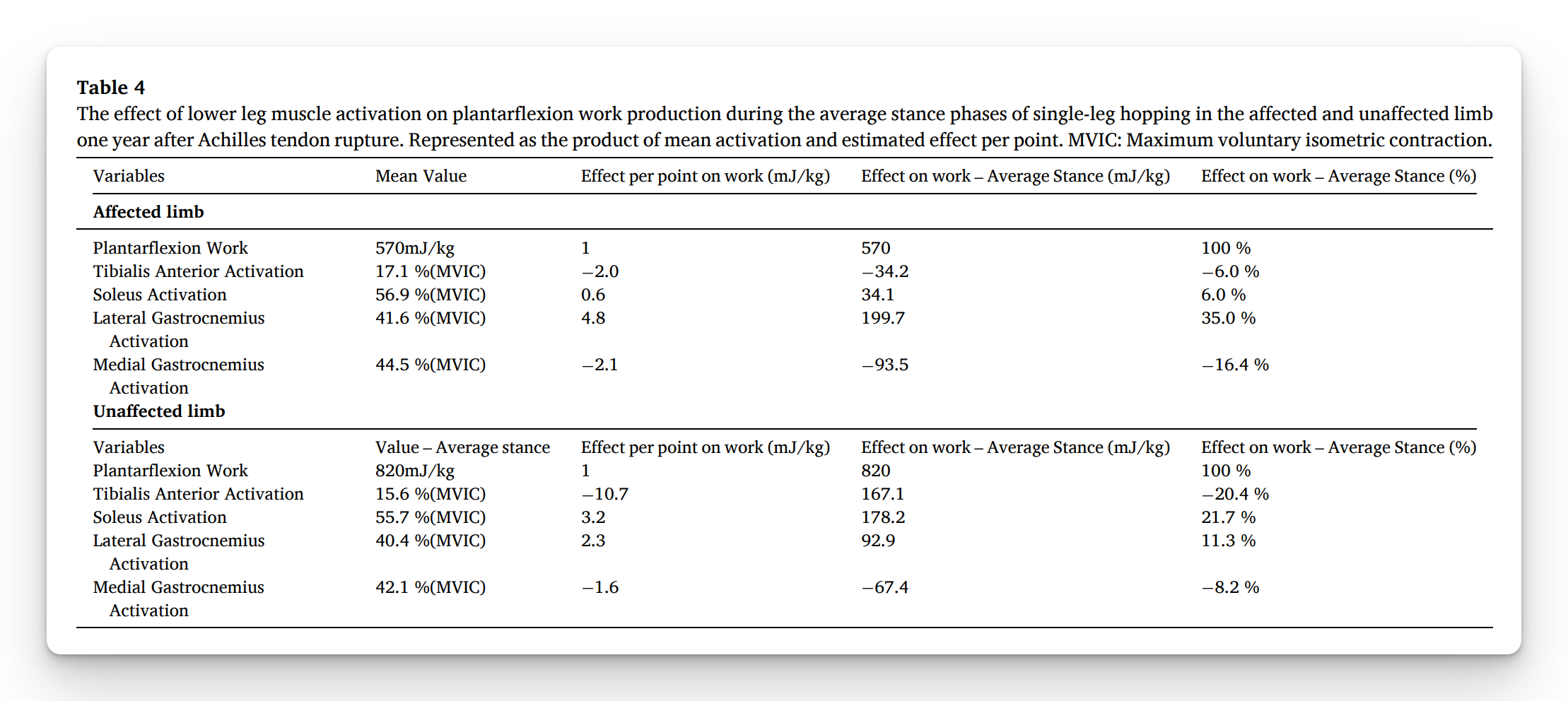
- Mixed effects linear model to determine how much each muscle’s activation contributed to ankle work
What Were the Results?
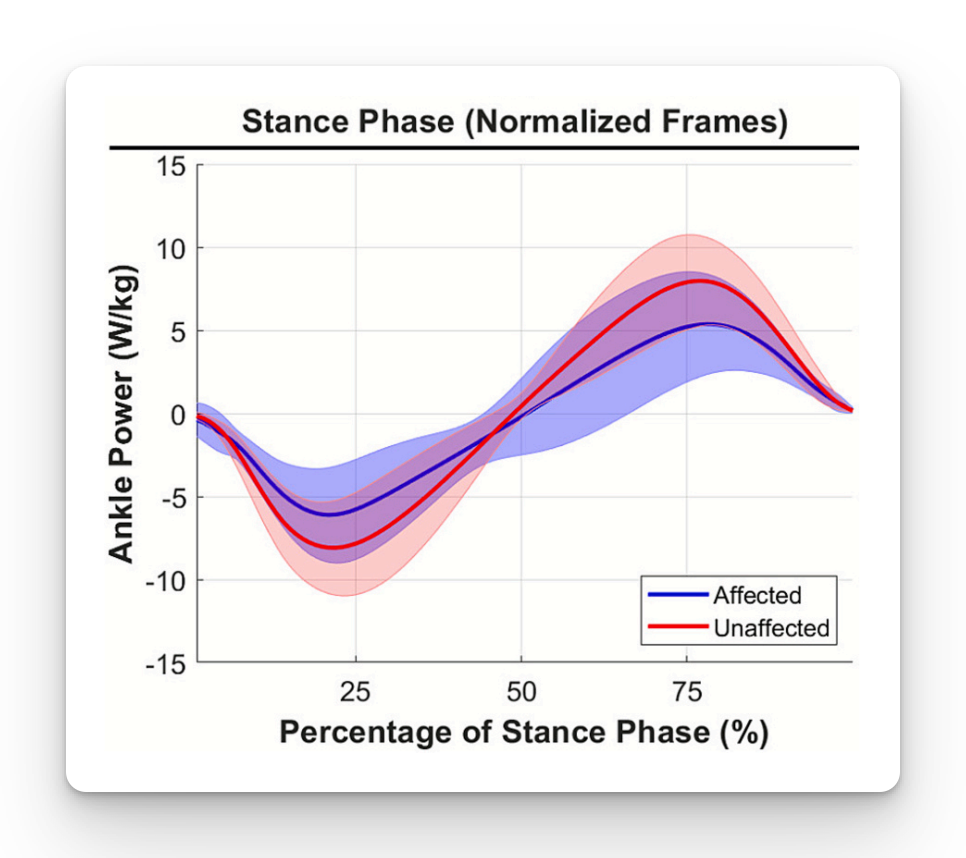
Plantarflexion Power Was Down
- 20–25% reduction in ankle power
- 42% reduction in plantarflexion work
- Significant deficits in both landing and push-off phases (p < 0.001)
Muscle Activation Did NOT Differ
- No side-to-side EMG differences for Soleus, Gastrocnemius (medial or lateral), or Tibialis anterior
- The muscles were turning on, they just weren’t producing the same work.
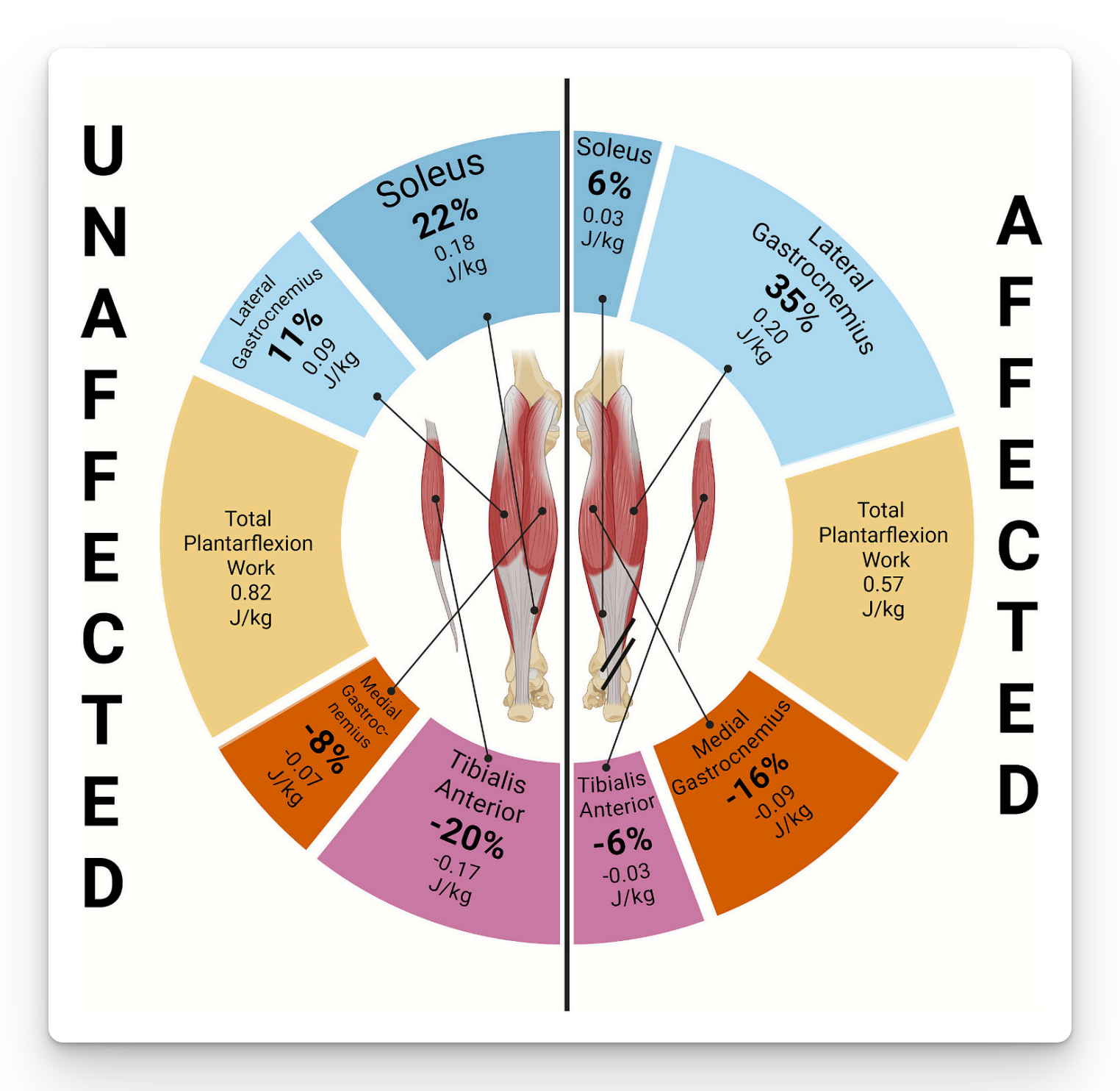
Contribution to Work Shifted
- For the soleus, the affected side had a ~81% reduction in effectiveness
- For the lateral gastroc, the affected side had ~108% increase in work
- The body shifted from monoarticular soleus dominance to biarticular gastroc reliance
What Does This Mean?
- This is a mechanical efficiency problem, likely driven by tendon elongation, fascicle shortening, reduced soleus cross-sectional area, and a shifted force–length operating range
- The biarticular gastrocnemius can transfer energy from the knee to the ankle, allowing it to compensate when the soleus underperforms
- The result is greater reliance on proximal-to-distal energy transport, meaning the system shifts work upstream to the knee extensors
Limitations
- Open hopping instructions increased variability
- No stratification by sex, treatment type, or age
- Cross-sectional design, no pre-injury baseline
Coach’s Takeaway
- EMG may look symmetrical, but plantarflexion work is still reduced, so don’t mistake muscle activity for true functional recovery
- The soleus contribution to plantarflexion work drops significantly post-rupture, so prioritize hypertrophy, long-duration isometrics, slow heavy strength work, and strategies that restore fascicle length
- The body shifts toward knee-driven compensation, so include eccentric gastroc work, knee-to-ankle energy transfer drills, and integrated plyometric progressions
I hope this helps,
Ramsey
Reference
Harðarson GR, Huseth KR, Aagaard P, et al. (2026). Differential contributions of lower leg muscle activation to plantar flexor function during single-leg hopping one year after Achilles tendon rupture: A shift from monoarticular to biarticular muscle work. Journal of Biomechanics, 195, 113082.


