

Achilles tendinopathy (AT) is common in athletes and active adults, and exercise is the cornerstone of care.
Yet programs vary in how they prescribe heel raises and related loading.
Coaches and clinicians need clarity on which exercise parameters move outcomes.
This modified Delphi gathered leading AT experts to rate and rank the heel raise exercise parameters that most influence rehab outcomes for midportion and insertional AT.
Which heel raise exercise parameters influence midportion and insertional AT rehabilitation outcomes?
What Did the Researchers Do?
The authors performed a three-round Delphi study with 17 international researcher-clinicians who publish on AT exercise rehab.
Task
- Experts rated 16 heel-raise parameters on their influence on outcomes, then ranked their importance.
- This was an expert panel, not patients; the target application is clinical practice with AT.
Variables Assessed
- Intensity of contraction, number of reps and sets, total time under tension (TUT), duration, tempo, loading rate, rest, pain during exercise, ROM details (dorsiflexion, plantarflexion), knee flexion, foot position/rotation, frequency, shoes vs no shoes, and contraction type.
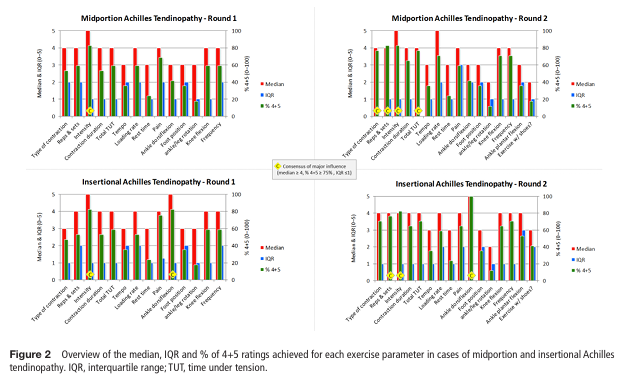
- Consensus criteria was median ≥4, ≥75% scoring 4–5, IQR ≤1.
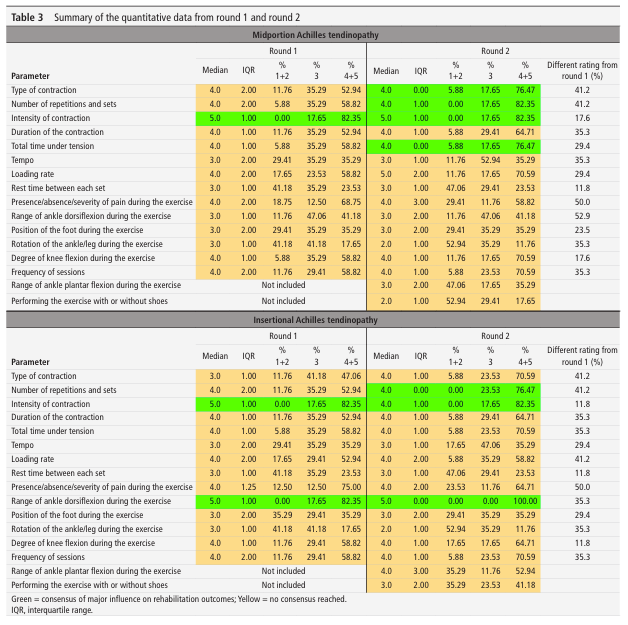
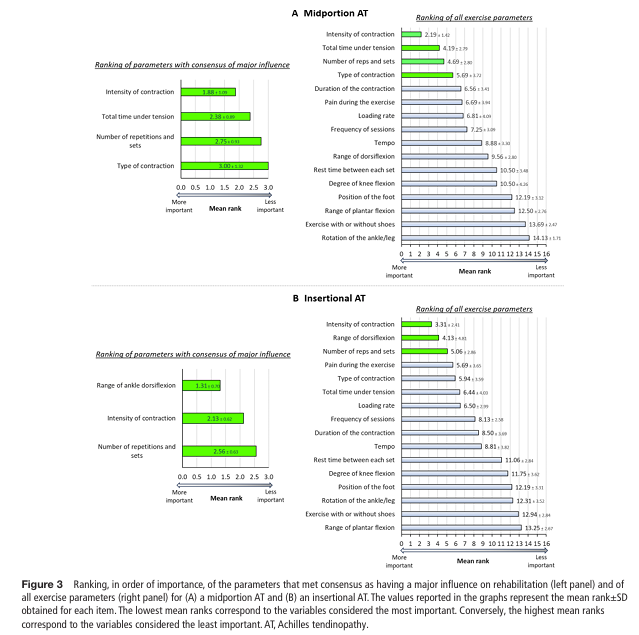
What were the results?
Midportion AT (Major Influence)
- Intensity of contraction (top), total TUT, reps and sets, and type of contraction.
Insertional AT (Major Influence)
- Range of ankle dorsiflexion (top), intensity of contraction, reps and sets.
Pain during exercise
- Pain ranked high overall but did not exceed the preset “major influence” consensus threshold, likely because pain serves as a regulator for dosing rather than a direct driver of tissue adaptation.
Plyometrics
- Plyometrics are essential, but typically introduced later due to high loads and short contraction times.
Programming
- Program duration and frequency matter for practice; however, this Delphi study targeted the how of each exercise, rather than the overall plan.
What Does This Mean?
Load It Like You Mean It
- For both subtypes, contraction intensity is a big lever.
- Heavier loading tends to align with the tendon strain range thought to drive adaptation, and it also builds calf strength for return to running and jumping.
Volume Matters, But Pick the Right Dial
- Reps and sets and total TUT earned consensus (TUT for midportion; near-consensus for insertional).
- Use them to ensure the tendon gets adequate time under meaningful tension.
Match ROM to Pathology
- For insertional AT, early rehab should limit dorsiflexion to reduce compressive stress at the calcaneal insertion, then reintroduce ROM gradually.
- For midportion, use fuller ROM as tolerated.
Comprehensive Contraction
- Include isometric, slow isotonic, and later plyometrics to restore function across the spectrum.
- Progress according to pain tolerance and functional improvement.
Limitations
- Expert opinion, not an RCT; some parameters have mixed or limited direct evidence.
- Parameters outside the exercise execution (eg, full program progression, psychosocial factors) were not the primary focus, though noted.
Coach’s Takeaway
- Prioritize intensity to hit meaningful tendon strain and build capacity.
- Dose with reps/sets and TUT to create sufficient stimulus without flaring symptoms.
- Respect location by limiting dorsiflexion early in insertional cases; use fuller ROM earlier in midportion.
- Progress to plyos once pain is stable and strength capacity has increased.
- Use pain as a dashboard, monitoring it during, after, and the next day to guide load.
I hope this helps,
Ramsey
Reference
Demangeot Y, O’Neill S, Degache F, et al. (2025). Exercise parameters to consider for Achilles tendinopathy: a modified Delphi study with international experts. British Journal of Sports Medicine. https://doi.org/10.1136/bjsports-2025-110183


